Section
5
Assessing Adiposity
Dual Energy X-Ray Absorptiometry (DXA)
The DXA method uses two low dose X-ray beams and instrument-specific algorithms to estimate total-body and regional estimates of body components, including bone mineral content, “bone-free” fat-free mass, and fat mass.108 This method can be used across all ages, from infancy through adulthood.
Procedure
The participant, wearing light clothing and with all metal removed from the body, lies flat on their back on the DXA stretcher, with feet pointed up and secured with a Velcro strap, and arms by the side and not overlapping any part of the body (Figure 14).
Figure 14: Dual Energy X-Ray Absorptiometry
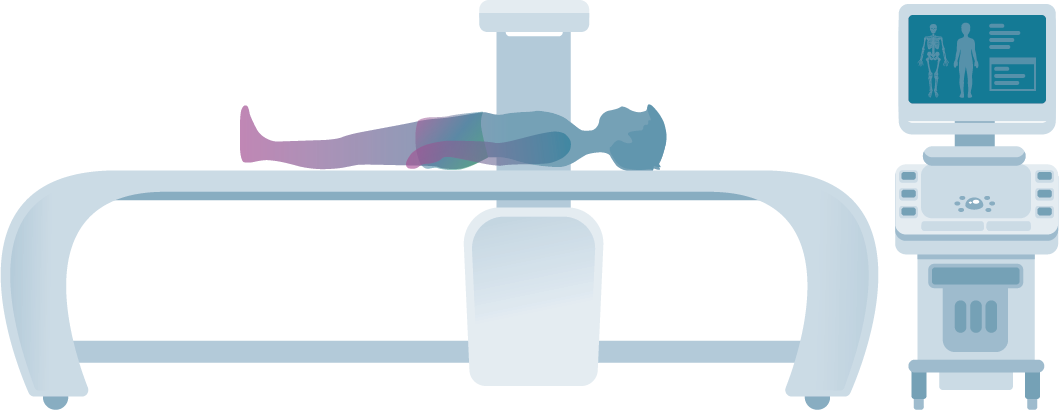
Persons whose body size extends to the field-of-view limit can be wrapped securely in a bed sheet to ensure that all soft tissue has been retained within the field of view. An invisible beam of low-dose X-rays with two distinct low- and high-energy level peaks is transmitted through the body. The measured attenuation of the two main energy peaks is used to estimate each pixel’s fraction of fat and lean mass. Fat and lean components are quantified over regions devoid of bone. Using specific anatomic landmarks from the whole-body scan, the trunk, legs, and arms are identified. The fat tissue in the arms and legs is largely subcutaneous fat. The fat-free soft tissue (i.e., non-fat and non-bone mineral mass) of the arms and legs is largely skeletal muscle.
Estimates of Body Fat, Interpretation, and Limitations
The dominant commercial DXA systems that supply body composition software are Hologic and GE Lunar. Instrument-specific software algorithms are used to calculate the various values for bone mineral content, “bone-free” lean mass or FFM, and FM, which are based on the differential absorption of X-rays of the two different energy levels by the different body components. The two systems generate different values for bone and soft tissue in the same person due to differences in technology detectors, calibration, bone edge detection, and reference data included in each system’s software. Given this, it is recommended that researchers use the same DXA software system when assessing body composition in the same individuals over time, such as in longitudinal studies and clinical trials. Similarly, upgrades in the hardware and software within the same DXA manufacturer’s system can result in different values on the same person. It is recommended that upgrades be avoided during longitudinal assessments on the same individuals, but if unavoidable, cross-validation studies need to be conducted to assess differences in values in the same individuals due to the upgrade in the system components.
Assumptions associated with DXA include (a) the assumed constant attenuation (R) of fat (R = 1.21) and of bone mineral content, (b) minimal effects of hydration on lean tissue estimates, and (c) lack of an effect of variations in regional (e.g., chest, leg, arm) thickness on soft tissue estimates109 and that the fat content of the area being analyzed (non-bone-containing area/pixels) is comparable to the fat content of the unanalyzed area (bone-containing area or pixels). When these assumptions are not met, errors occur in the estimation of fat, lean, and bone in both regional and whole-body values. Scenarios when assumptions may not be met include when trunk tissue thickness or depth is high (as in extreme obesity) and clinical states where hydration is abnormal.
Validity and Reliability
In adults, DXA estimates of FM correlate highly with other established methods for accurately assessing body FM such as in-vivo neutron activation analysis (IVNA)110 and in children aged 6–18 years when compared to under water weighing.49 DXA estimates of FM are influenced by “trunk thickness,” with the error increasing as the subject’s trunk thickness increases.
Reference Data
National reference data are available in the U.S. population aged 8–85 years. During the years 1999–2004, the National Health and Nutrition Examination Survey (NHANES) study acquired whole-body DXA scans on a population-based sample of Americans aged 8–85 years using the Hologic DXA systems. Using this system, national reference values were generated for total and sub-total whole-body results11,12 and were normalized to age, height, or lean mass.33 NHANES reference values were later derived from these data for use with the GE Healthcare Lunar DXA systems.111
Accessibility, Training, and Cost
Accessibility to DXA systems tends to be low to moderate. A whole-body DXA scan for the determination of body composition is primarily available at research laboratories and radiology/hospital facilities with DXA equipment containing whole-body composition software. However, even if a facility has access to a DXA system, it does not mean it contains the software to conduct a body composition scan. DXA systems may be programmed to conduct bone density scans and may require additional software to be used for body composition analyses. Due to the low-dose radiation, the equipment also has special storage room requirements, and a certified radiology technician or physician is required to operate the scanner. Equipment is expensive when first purchased ($80,000), and the annual cost of a service contract is high ($8,000–$13,000).
Acceptability, Participant Burden, and Risk
Acceptability is moderate and risk is minor, due to the low-dose ionizing radiation exposure. The dose from a single whole-body scan is generally < 10 microSieverts.112 This is equivalent to a single day’s exposure from natural sources at sea level such as from the sun, ground, and water. Burden for the study participant is low, and the measure is generally noninvasive. Participants who may be pregnant should not be measured, and pregnancy screening is required. In addition, the scanning bed or stretcher of most models has an upper weight limit (Hologic 159 kg; GE 182 kg) and the whole-body field of view cannot accommodate persons with body weights greater than this limit. The Norland Elite is a newer model that has been designed for whole body composition and can scan larger individuals (283.5 kg (625 lb), 137 cm (54”) wide and 228 cm (7′6”) tall). Because participants are required to remain motionless during the procedure, and sedation is generally not permitted for research studies, special consideration must be given to immobilizing/restraining infants and young children to prevent movement, especially after 6 months of age, which may limit feasibility. The time to complete the scan varies with the size and compliance of the participant but is generally 10–20 minutes.
Summary
DXA is a relatively more resource-intensive and costly method that is reasonably short in duration. It is generally safe and noninvasive but has a very low-dose ionizing radiation exposure that may limit its acceptability. It requires certified technicians and is not portable and often is only available in clinical/radiology facility settings. People undergoing this measurement must be motionless, and restraints may be required to maintain immobility, limiting its use for many children.